Abdominal hysterectomy
- Description
- Faq's
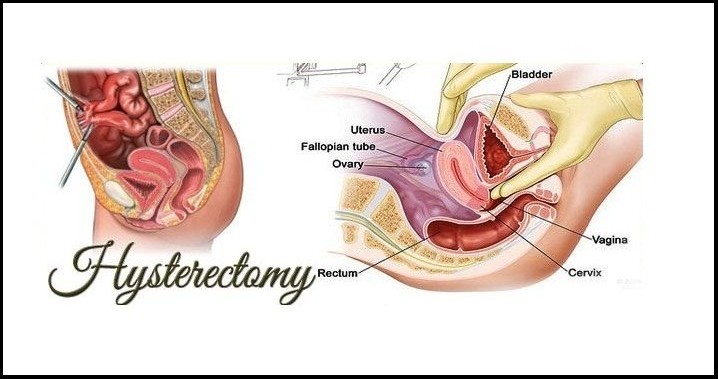
An abdominal hysterectomy is a surgical procedure that removes your uterus through an incision in your lower abdomen. Your uterus — or womb — is where a baby grows if you're pregnant. A partial hysterectomy removes just the uterus, leaving the cervix intact. A total hysterectomy removes the uterus and the cervix.
Sometimes a hysterectomy includes removal of one or both ovaries and fallopian tubes, a procedure called a total hysterectomy with salpingo-oophorectomy (sal-ping-go-o-of-uh-REK-tuh-me).
A hysterectomy can also be performed through an incision in the vagina (vaginal hysterectomy) or by a laparoscopic or robotic surgical approach — which uses long, thin instruments passed through small abdominal incisions.
An abdominal hysterectomy may be recommended over other types of hysterectomy if:
- You have a large uterus.
- Your doctor wants to check other pelvic organs for signs of disease.
- Your surgeon feels it's in your best interest to have an abdominal hysterectomy.
You may need a hysterectomy to treat:
- Gynecologic cancer. If you have a gynecologic cancer — such as cancer of the uterus or cervix — a hysterectomy may be your best treatment option. Depending on the specific cancer you have and how advanced it is, your other options might include radiation or chemotherapy.
- Fibroids. A hysterectomy is the only certain, permanent solution for fibroids — benign uterine tumors that often cause persistent bleeding, anemia, pelvic pain or bladder pressure. Nonsurgical treatments of fibroids are a possibility, depending on your discomfort level and tumor size. Many women with fibroids have minimal symptoms and require no treatment.
- Endometriosis. In endometriosis, the tissue lining the inside of your uterus (endometrium) grows outside the uterus on your ovaries, fallopian tubes, or other pelvic or abdominal organs. When medication or conservative surgery doesn't improve endometriosis, you might need a hysterectomy along with removal of your ovaries and fallopian tubes (bilateral salpingo-oophorectomy).
- Uterine prolapse. Descent of the uterus into your vagina can happen when supporting ligaments and tissues weaken. Uterine prolapse can lead to urinary incontinence, pelvic pressure or difficulty with bowel movements. A hysterectomy may be necessary to treat these conditions.
- Abnormal vaginal bleeding.If your periods are heavy, irregular or prolonged each cycle, a hysterectomy may bring relief when the bleeding can't be controlled by other methods.
- Chronic pelvic pain. Occasionally, surgery is a necessary last resort for women who experience chronic pelvic pain that clearly arises in the uterus. However, a hysterectomy provides no relief from many forms of pelvic pain, and an unnecessary hysterectomy may create new problems. Seek careful evaluation before proceeding with such major surgery.
A hysterectomy ends your ability to become pregnant. If you think you might want to become pregnant, ask your doctor about alternatives to this surgery. In the case of cancer, a hysterectomy might be the only option. But for other conditions — including fibroids, endometriosis and uterine prolapse — you may be able to try less invasive treatments first.
During hysterectomy surgery, your surgeon might also perform a related procedure that removes both of your ovaries and your fallopian tubes (bilateral salpingo-oophorectomy). You and your doctor should discuss ahead of time whether you need this procedure, which results in what's known as surgical menopause. With surgical menopause, menopause symptoms often begin suddenly for women after having the procedure done. Depending on how much these symptoms affect your quality of life, you may need short-term treatment with hormones. RisksA hysterectomy is generally very safe, but with any major surgery comes the risk of complications.
Risks associated with an abdominal hysterectomy include:
- Blood clots
- Infection
- Excessive bleeding
- Adverse reaction to anesthesia
- Damage to your urinary tract, bladder, rectum or other pelvic structures during surgery, which may require further surgical repair
- Earlier onset of menopause even if the ovaries aren't removed
- Rarely, death
It's normal to feel anxious about having a hysterectomy. Here's what you can do to prepare:
- Gather information. Before surgery, get all the information you need to feel confident about your decision to have a hysterectomy. Ask your doctor and surgeon questions. Learn about the procedure, including all the steps involved if it makes you feel more comfortable.
- Follow your doctor's instructions about medication. Find out whether you should change your usual medication routine in the days leading up to your hysterectomy. Be sure to tell your doctor about any over-the-counter medications, dietary supplements or herbal preparations that you're taking.
- Discuss what type of anesthesia you'll have. Abdominal hysterectomy requires you to have general anesthesia, which makes you unconscious during surgery.
- Plan for a hospital stay. How long you'll be in the hospital depends on what type of hysterectomy you have and what your doctor recommends. Generally, abdominal hysterectomy requires a hospital stay of at least one to two days.
- Arrange for help. Full recovery could take several weeks. Your doctor may recommend restricting your activities during your recovery, such as avoiding driving or lifting heavy objects. Arrange for help at home if you think you'll need it.
